


Prehospital Blood Transfusion
Prehospital blood transfusion is the delivery of whole blood or blood components (packed red blood cells, plasma, platelets) by EMS clinicians to a patient who is bleeding severely, internally or externally. This care can be administered at the scene of injury and/or en route to definitive medical care.
NHTSA’s commitment to reducing roadway deaths and disability through post-crash care—part of a Safe System Approach—includes finding innovative ways to save lives that would otherwise be lost in a motor-vehicle crash. The rapid expansion of prehospital blood transfusion programs at EMS agencies around the country is an important part of reducing the number of fatalities.
How Prehospital Blood Transfusion Saves Lives
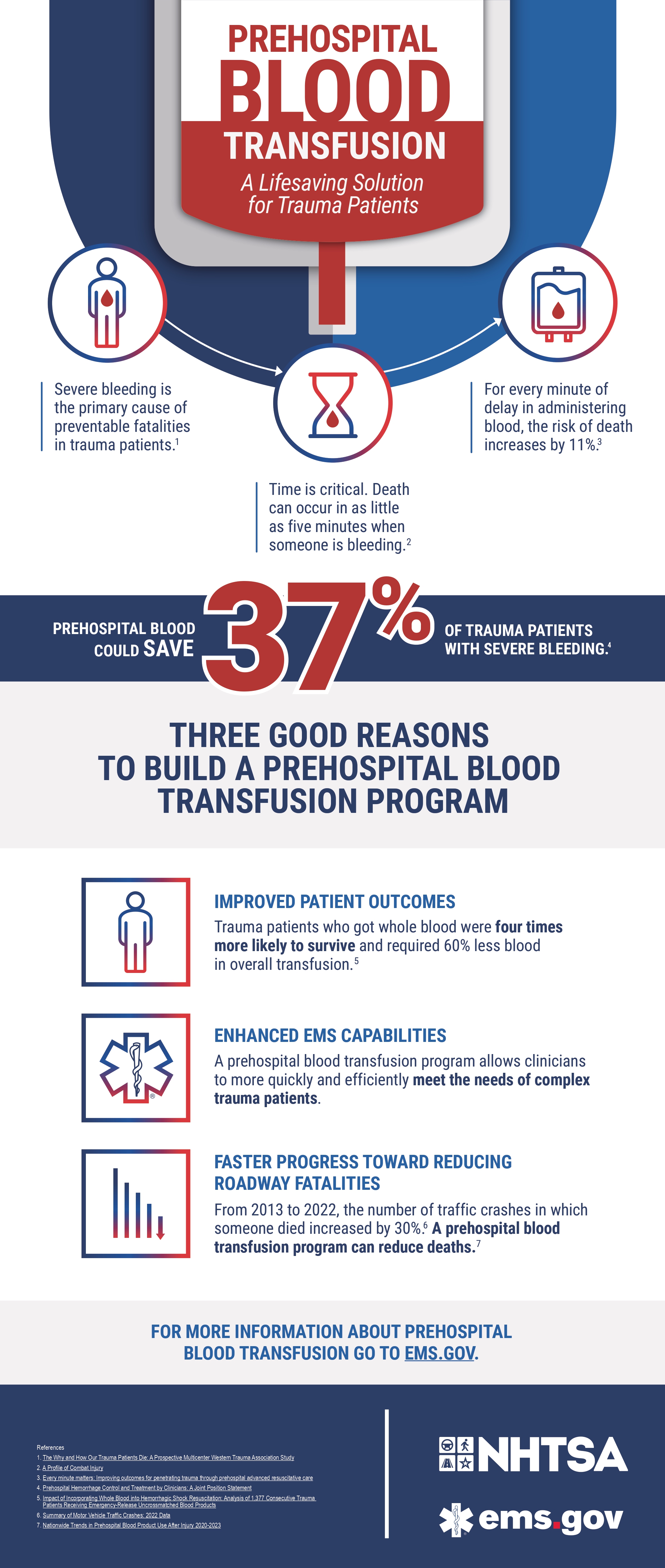
Severe bleeding is the primary cause of preventable fatalities in trauma patients, including those involved in a motor-vehicle crash. But with the prompt delivery of prehospital blood or blood products, it’s estimated that 37% of trauma patients with severe bleeding could be saved. For every minute of delay in administering blood, the risk of death increases by 11%.
The Benefits of Establishing a Prehospital Blood Program
By bringing whole blood or component therapy to the point of injury, EMS teams can act faster to stabilize critical patients and ultimately save more lives. Here are three key benefits:
Improved patient outcomes – Trauma patients who received whole blood in the field were four times more likely to survive than those who did not.
Enhanced EMS capabilities – A prehospital blood transfusion program allows clinicians to more quickly and efficiently stabilize complex trauma patients.
Faster progress toward reducing roadway fatalities – Between 2013 and 2022, fatal traffic crashes increased by 30%. As trauma-related deaths rise, giving emergency responders the ability to administer blood before patients reach the hospital can significantly improve survival rates.
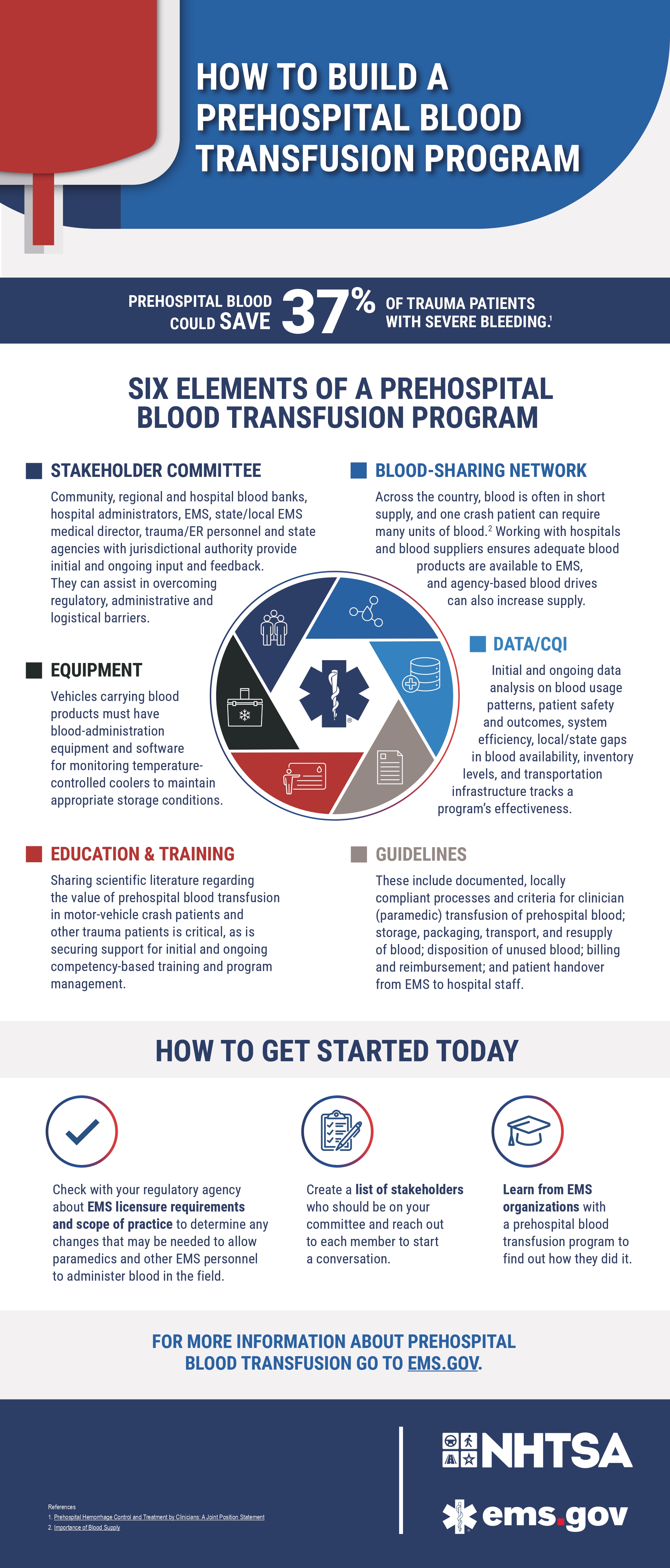
The Six Elements of a Prehospital Blood Transfusion Program
-
Community, regional and hospital blood banks, hospital administrators, EMS, state/local EMS medical director, trauma/ER personnel and state agencies with jurisdictional authority provide initial and ongoing input and feedback. They can assist in overcoming regulatory, administrative and logistical barriers. 911 telecommunicators, who can deliver emergency medical dispatch protocols related to deploying blood, should also be part of early conversations when setting up an EMS prehospital blood transfusion program.
-
Across the country, blood is often in short supply, and one crash patient can require many units of blood. Working with regional hospitals and blood banks ensures adequate blood products are available to EMS, and agency-based blood drives can also increase supply.
-
Vehicles carrying blood products must have blood-administration equipment and software for monitoring temperature-monitored coolers to maintain appropriate storage conditions.
-
Sharing scientific literature supporting the value of prehospital blood transfusion in motor-vehicle crash patients and other trauma patients is critical, as is securing support for initial and ongoing competency-based training and program management.
-
Initial and ongoing data analysis on blood usage patterns, patient safety and outcomes, system efficiency, local/state gaps in blood availability, inventory levels, and transportation infrastructure tracks a program’s effectiveness.
-
These include documented, locally compliant processes and criteria for clinician (paramedic) transfusion of prehospital blood; storage, packaging, transport and resupply of blood; disposition of unused blood; billing and reimbursement; and patient handover from EMS to hospital staff.